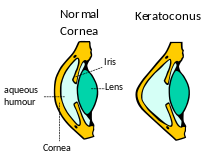
Keratoconus (KC) is a disorder of the eye which results in progressive thinning of the cornea over time. This can result in blurry vision, double vision, astigmatism, and light sensitivity. Usually both eyes are affected though one eye can be much more advanced than the other.
Keratoconus affects about 1 in 2,000 people. It occurs most commonly in late childhood to early adulthood. While it occurs in all populations it may be more frequent in certain ethnic groups such as those of Asian descent. The word is from the Greek kéras meaning cornea and the Latin cōnus meaning cone.
Eye rubbing and childhood eye allergies play a role in the development of keratoconus. The underlying mechanism involves changes of the cornea to a cone shape.
Keratoconus affects about 1 in 2,000 people. It occurs most commonly in late childhood to early adulthood. While it occurs in all populations it may be more frequent in certain ethnic groups such as those of Asian descent. The word is from the Greek kéras meaning cornea and the Latin cōnus meaning cone.
Signs and Symptoms

Simulation of the multiple images seen by a person with keratoconus.
People with early keratoconus typically notice a minor blurring of their vision and come to their clinician seeking corrective lenses for reading or driving. The vision can get progressively worse and the patient notices that even with frequent change glasses the vision isn’t improving. As the disease advances photophobia (sensitivity to bright light) and eye strain from squinting in order to read are common.
The classic symptom of keratoconus is the perception of multiple “ghost” images, known as monocular polyopia. The visual distortion experienced by the person comes from two sources, one being the irregular deformation of the surface of the cornea, and the other being scarring that occurs on it. These factors act to form regions on the cornea that map an image to different locations on the retina.